
I was part of something new last week. It is perhaps the first time this was done in India.
A 4 year old girl was referred to me after she recovered from a fall from the second floor on to a cement road. She came to me with a strange complaint from her parents. Whenever the child cried, the left side of the face would swell up. She had Rhinorrhoea (running nose) and frequent headaches.

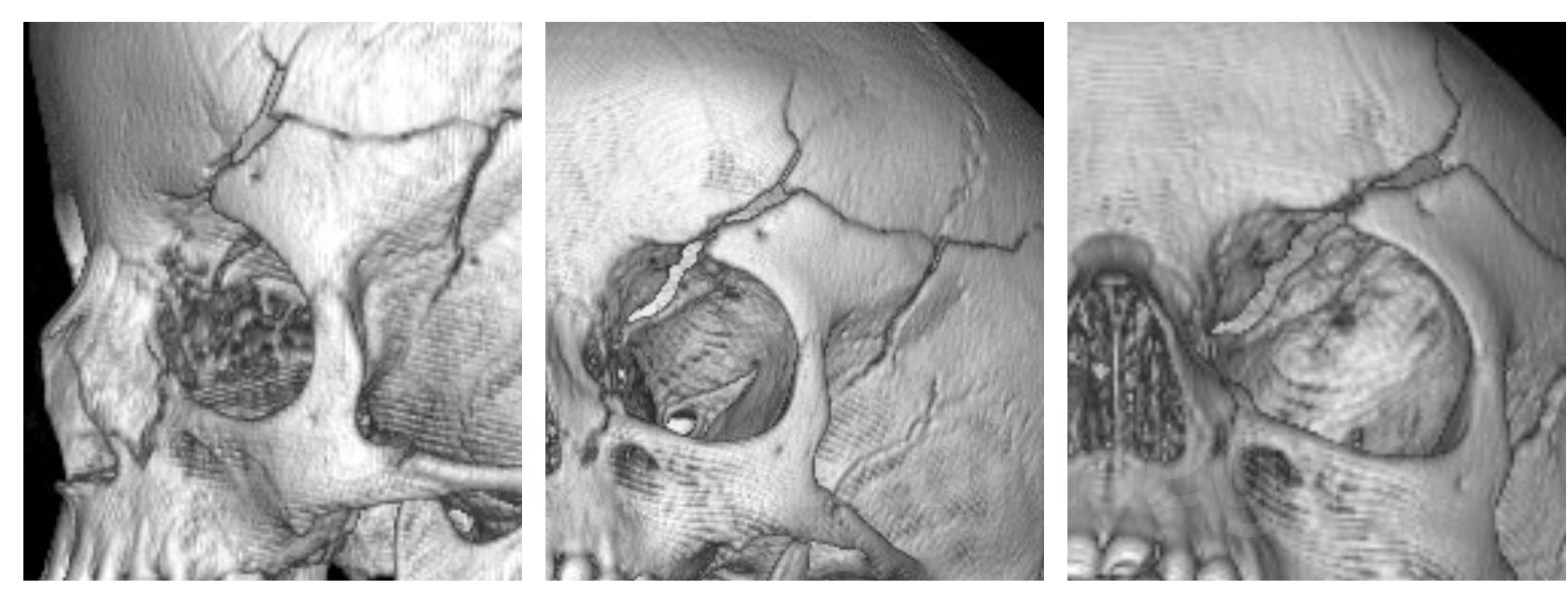
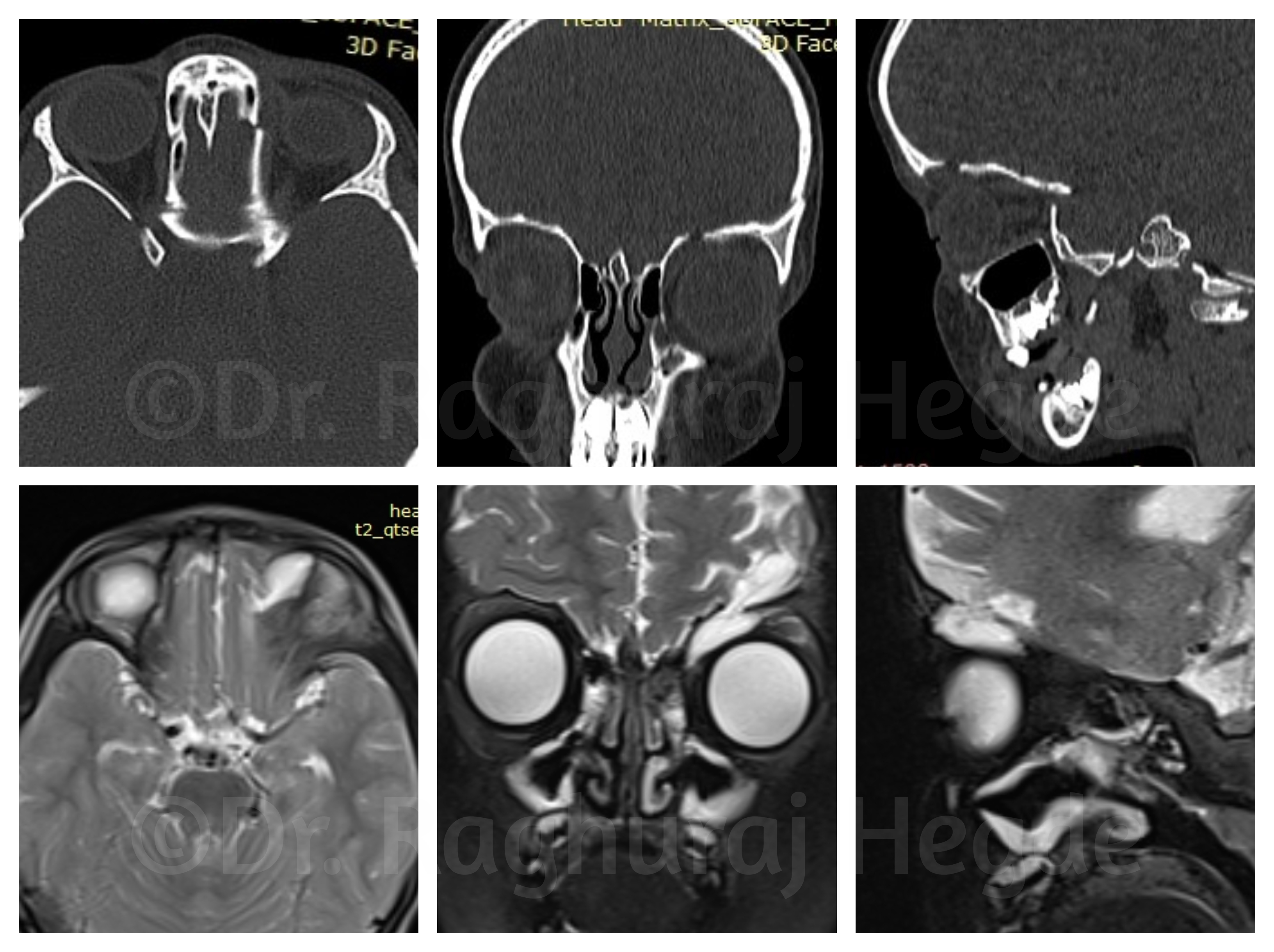
Her CT Scan showed why it was so.

She had crack in her skull starting from her Left ethmoid sinus passing through her left orbit superiorly into the frontal bone- a huge ugly crack. There was a direct tract from the sinuses to the subcutaneous space. Whenever she cried the increased sinus pressure would force air into the orbit and then into the skin which would be seen as a swelling. It was the cause of subcutaneous emphysema. The coronal, saggital and axial cuts confirmed the course of the orbito-frontal- cranial fracture line.

However on examination something didn’t make sense- the hypoglobus- pushing the left eye down. I carefully scouring the CT scan DICOM data in my computer from which I couldn’t pin-point a reason despite a left orbital roof defect.
To rule out a CSF leak, I ordered an MRI scan with contrast. On the scans it was imediately made clear that there was a meningoencephalocele into the left orbit. There was possibly a dural tear and CSF leak from that tear itself.
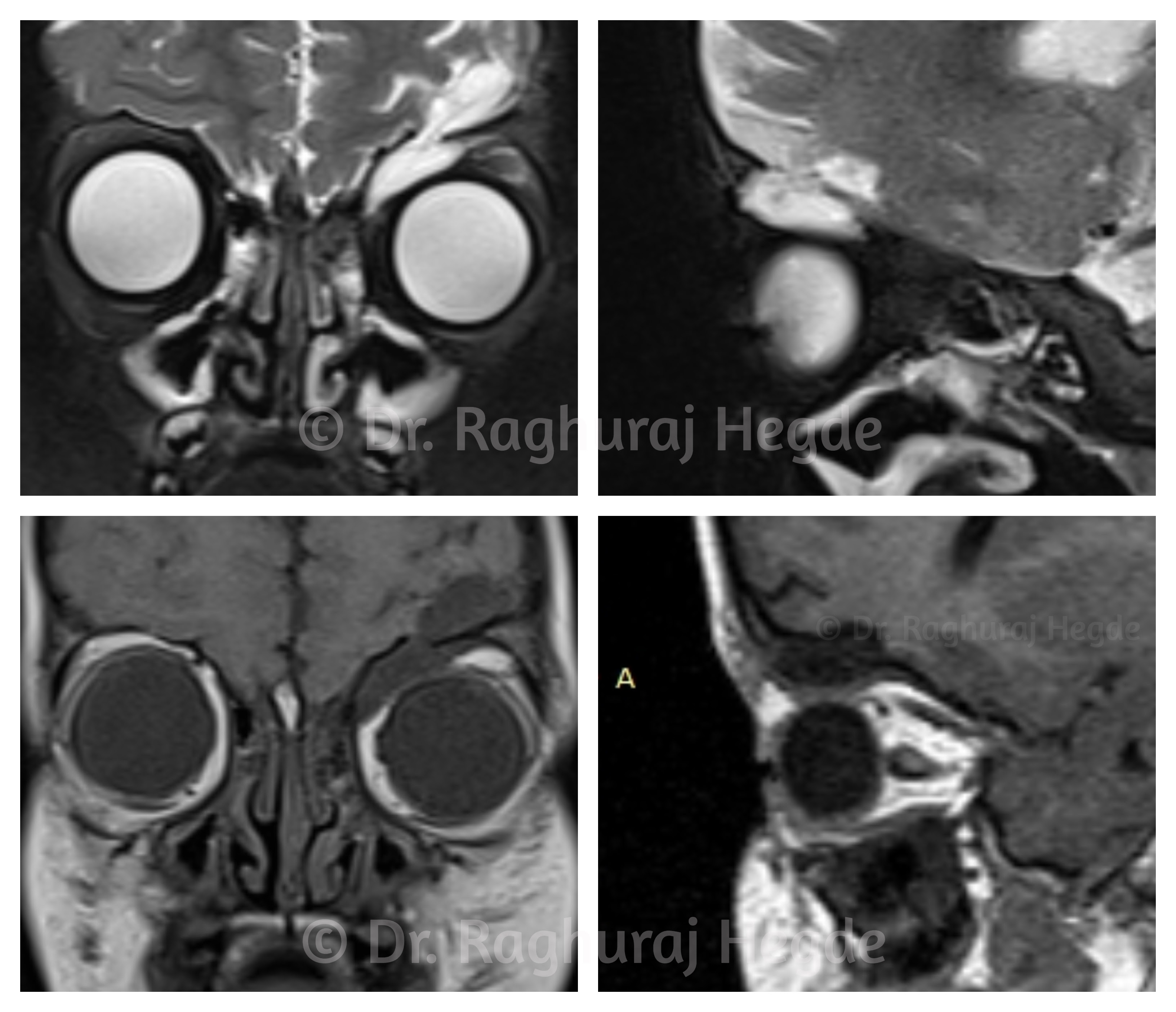
Correlating the CT scans with the MRI showed that the meningocele was through the left orbital roof defect.
Leaving it well alone would risk a future ascending infection. Even 6 months earlier, I would have referred this case to a neurosurgeon who would repair this with an open sky craniotomy and a bad scalp wound. That was the conventional treatment for such conditions.
I discussed this case with my colleague and skull base surgeon- Dr. Gaurav Medikeri. We have been collaborating with each other for a few cases in the last few months. As a team, we are exploring the possibility to approach the Anterior Cranial Fossa (ACF) using an orbital access- Trans-Orbital Neuro-Endoscopic Surgery (TONES). With this technique we can operate on skull base lesions with minimally invasive approach. This has the benefit of reduced morbidity, complications as well as hospital stay. I wanted to explore if there was a less invasive way to resolve the problem for this girl.
Since the patient was poor we managed to arrange for some funds from the charitable foundation of the hospitals we work in. Given the complexity of the case, we did a thorough planning for the surgery.
The surgery
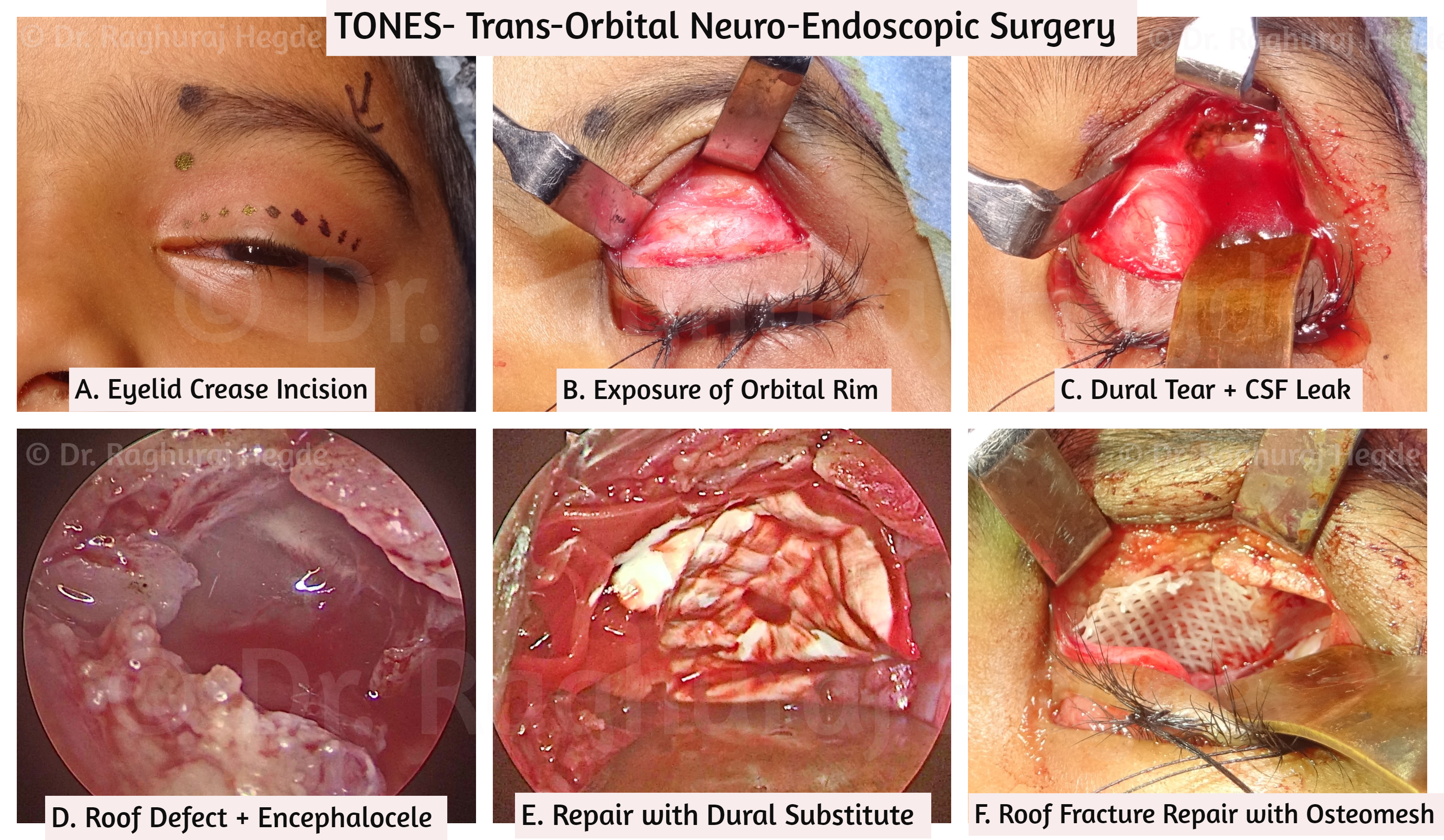
Trans-Orbital Neuro-Endoscopic Surgery (TONES)
We managed to fix this post-traumatic meningoencephalocele via TONES. I accessed the superior orbit and roof fracture through the upper eyelid crease incision dissecting in the sub-orbicularis pre-septal plane followed by a periosteal incision on the superior orbital rim. A gush of Cerebro-Spinal Fluid (CSF) burst through when I tried to separate the edges of the rood fracture from the prolapsed menigocele. The dural tear was larger than we had anticipated and dura was stuck to the peri-orbita. The arachanoid layer of the meninges was intact. The encephalocele had retracted from the orbital roof defect once the separation was done. My colleague then repaired the dural tear and CSF leak with a dural substitute. I then repaired the orbital roof fracture with osteomesh- an osteo-integrating mesh implant. New bone formation should occur in 1-2 years.
By doing this surgery using this technique, we managed to avoid a craniotomy and the accompanying scar in a 4 year old child. Her only scar from the surgery would be hidden in the eyelid crease.
With good planning and multi-disciplinary team work we can push boundaries while getting best outcomes for our patients. It is always exciting to do new things.
Update: March 2021
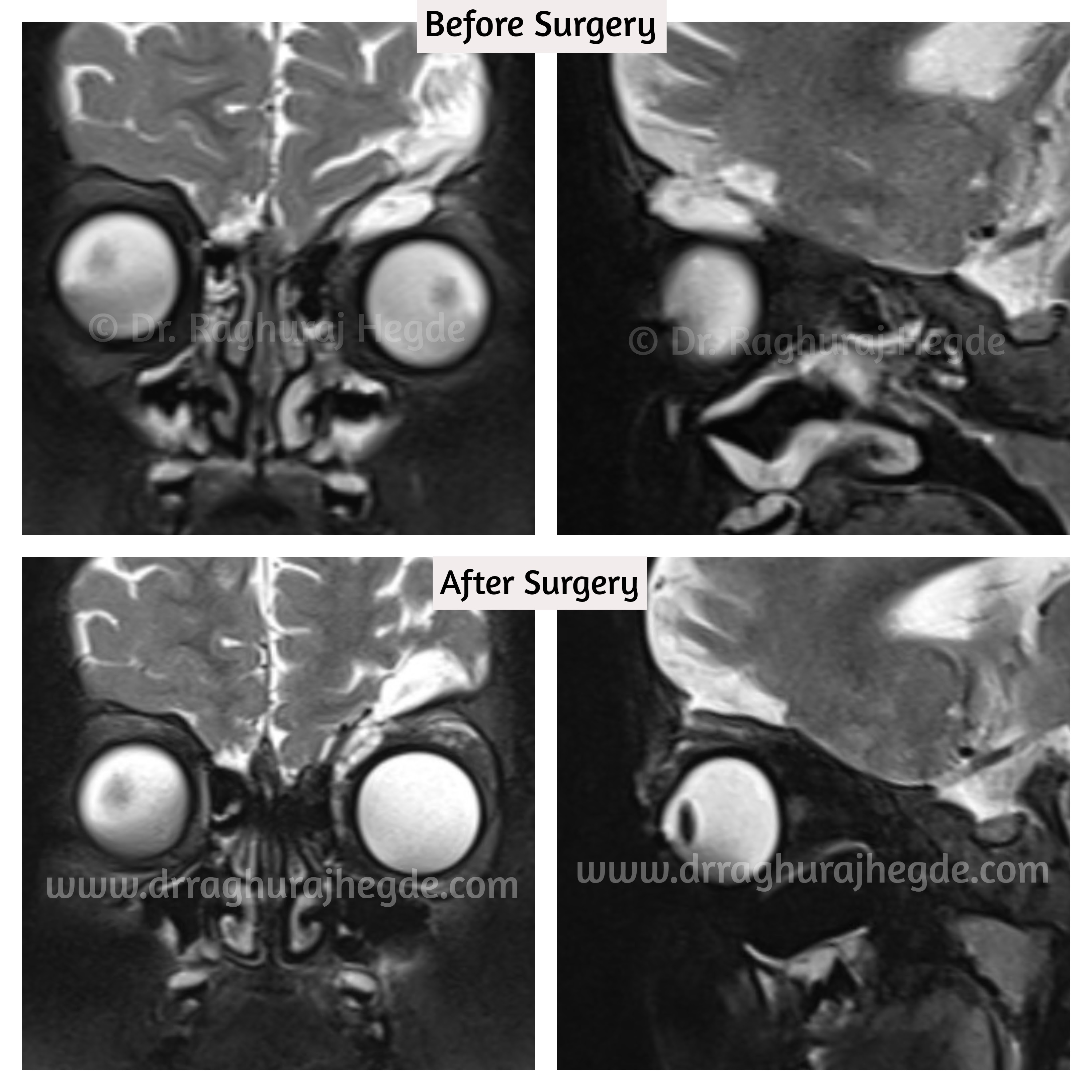
Wanted to update this case with post operative outcome and imaging photos.
About 8 weeks out from surgery, the child is doing well. The CSF Rhinorrhoea, headaches and hypoglobus has resolved. The sub-cutaneous emphysema has about 90% resolved and only the nasal area is getting filled up and not much of a problem. She has Left orbital residual enophthalmos resulting in left Pseudo-ptosis.

The post operative MRI imaging reveals that roof defect repair is successful and there is no proplapse of intra-cranial contents to the left orbit anymore.

As of now, we have decided not to chase after the left orbital enophthalmos and ptosis and wait for the tissues to recover from surgery. We will probably revisit the residual conditions at a later date.
©All patient photos are being used with the express consent of the patient. These cannot be shared or reproduced elsewhere.
