
This 22 year old school teacher was born with a condition called Blepharophimosis Syndrome. It is a rare congenital condition where the eyelids are not fully developed. It is characterised by Blepharophimosis– shortened vertical and horizontal palpebral fissures (eyelid openings), low/flat nasal bridge, Telecanthus (increased distance between the inner corners of the eyes making the eyes spaced widely apart), Ptosis (droopy eyelids). This condition is challenging to treat but amenable to treatment by surgery.
It involves a two stage surgery.
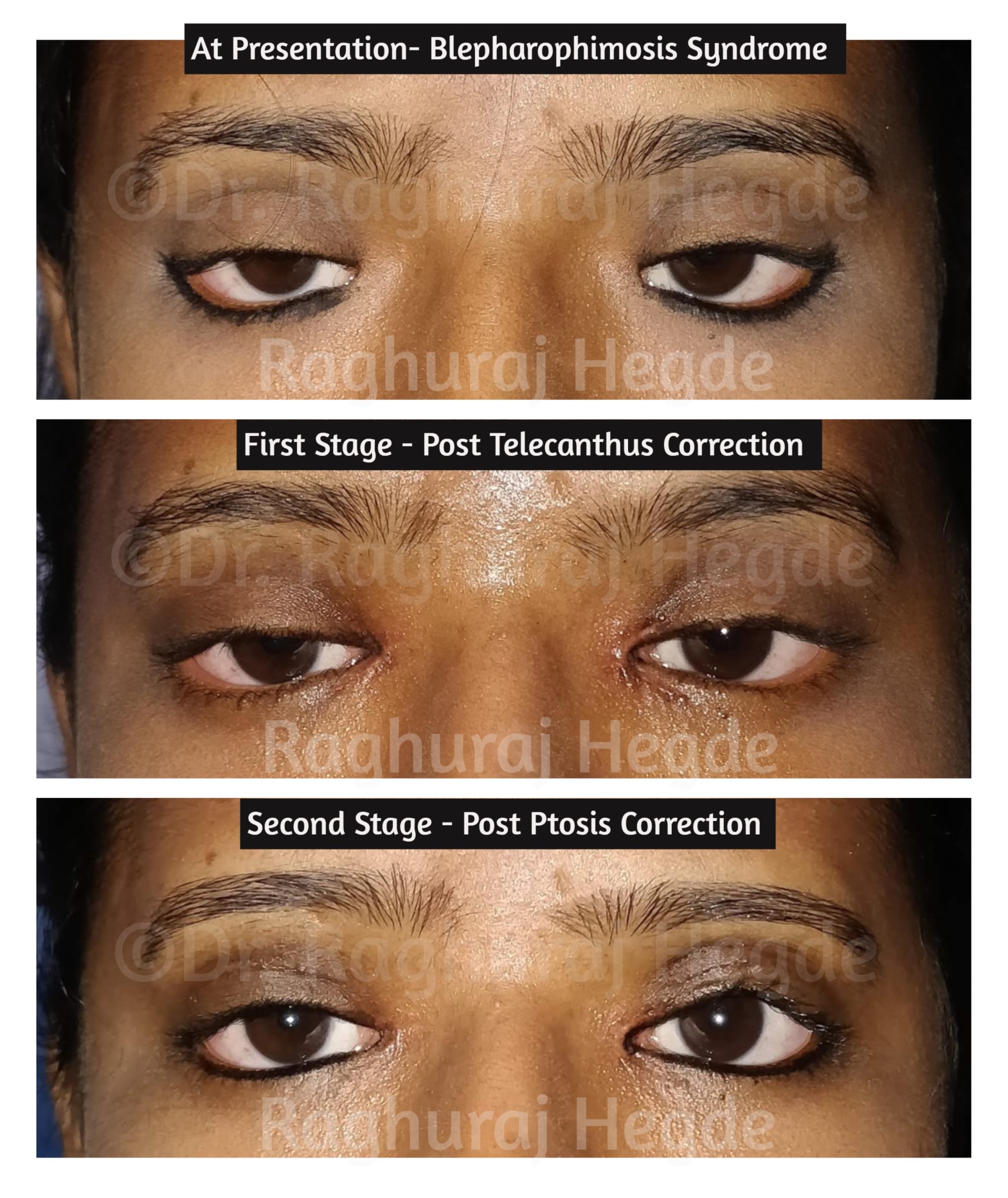
Stage 1 is the correction of the telecanthus followed about 4 weeks later with stage 2- ptosis correction.
In this case,
Stage 1- Telecanthus correction was done using a newer technique of medial epicanthoplasty described by Dr. Kim Yoon-Duck from Korea which I found superior to the traditional Mustarde’s double Z plasty. Other techniques include Y-V flap, Five Flap, Hornblass C to U Flap which usually involves multiple small flaps and high amount of scarring. This new technique involves a modified skin redraping method.This reduces the incidence of scarring due to lower number of incision lines as well as re-distributing the wound tension at medial canthus to the sub-ciliary incision line. The Telecanthus can be corrected by shortening the elongated medial canthal tendon and refixing it to the desired position. [1]
Stage 2- Ptosis correction was a bilateral levator resection surgery as she had moderate function of the levator palpebrae superioris (muscle which lifts the eyes).
Some surgeons prefer to do both stages at the same sitting. However I prefer to do it as a two stage procedure as it gives best outcomes in my hands.
Blepharophimosis syndrome is also knows as BPES (Blepharophimosis, Ptosis, Epicanthus Inversus Syndrome). It is an autosomal dominant condition usually inherited from parents but not always. The anomaly can be traced down to dysfunction or absence of the FOXL2 gene product which is expressed in the developing eyelids and ovaries. It is sometimes associated with other anomalies in the face such as lower lid ectropion, hypertelorism (increased distance between eye sockets) and lop ears. It is also sometimes associated with Premature Ovarian Insufficiency but expression varies.[2]
A big thanks to Dr. Stephanie Young (a former colleague and a very good friend) who suggested the new technique for medical epicanthoplasty used by her mentor in Korea- Dr. Kim Yoon-Duck. We oculoplastic surgeons discuss challenging cases among us using our collective experience to get the best outcomes for our patients.
The picture shows top to down at presentation(top), after stage 1 (middle) and final outcome (bottom). The end result is a wonderful outcome both functionally as well as cosmetically. Needless to say that the patient was happy as well as confident when she went to teach her class. :-).
References:
[1] Sa HS, Lee JH, Woo KI, Kim YD. A new method of medial epicanthoplasty for patients with blepharophimosis ptosis-epicanthus inversus syndrome. Ophthalmology. 2012;119:2402–7

Perfect
LikeLike