
Carotid-Cavernous Fistula
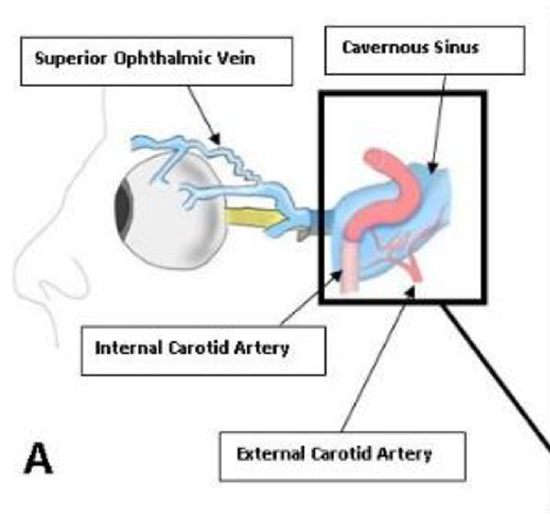
Carotid-Cavernous Fistula (CCF) is an abnormal passage of blood between the venous cavernous sinus and the internal carotid artery.
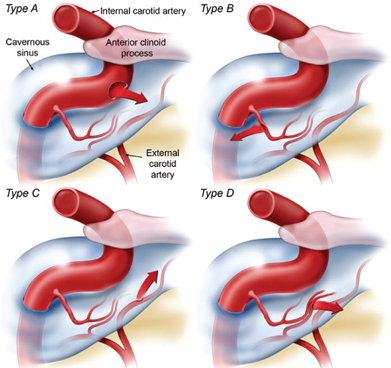
There are two main types of CCF as per the Barrow’s Classification (see pic below)
1. Direct CCFs or Type A where a tear in the internal carotid wall causes a single high flow fistula drains directly into the cavernous sinus.
2. Indirect CCFs or Type B,C,D- which are low-flow fistulas between meningeal branches of the internal carotid artery system and the cavernous sinus
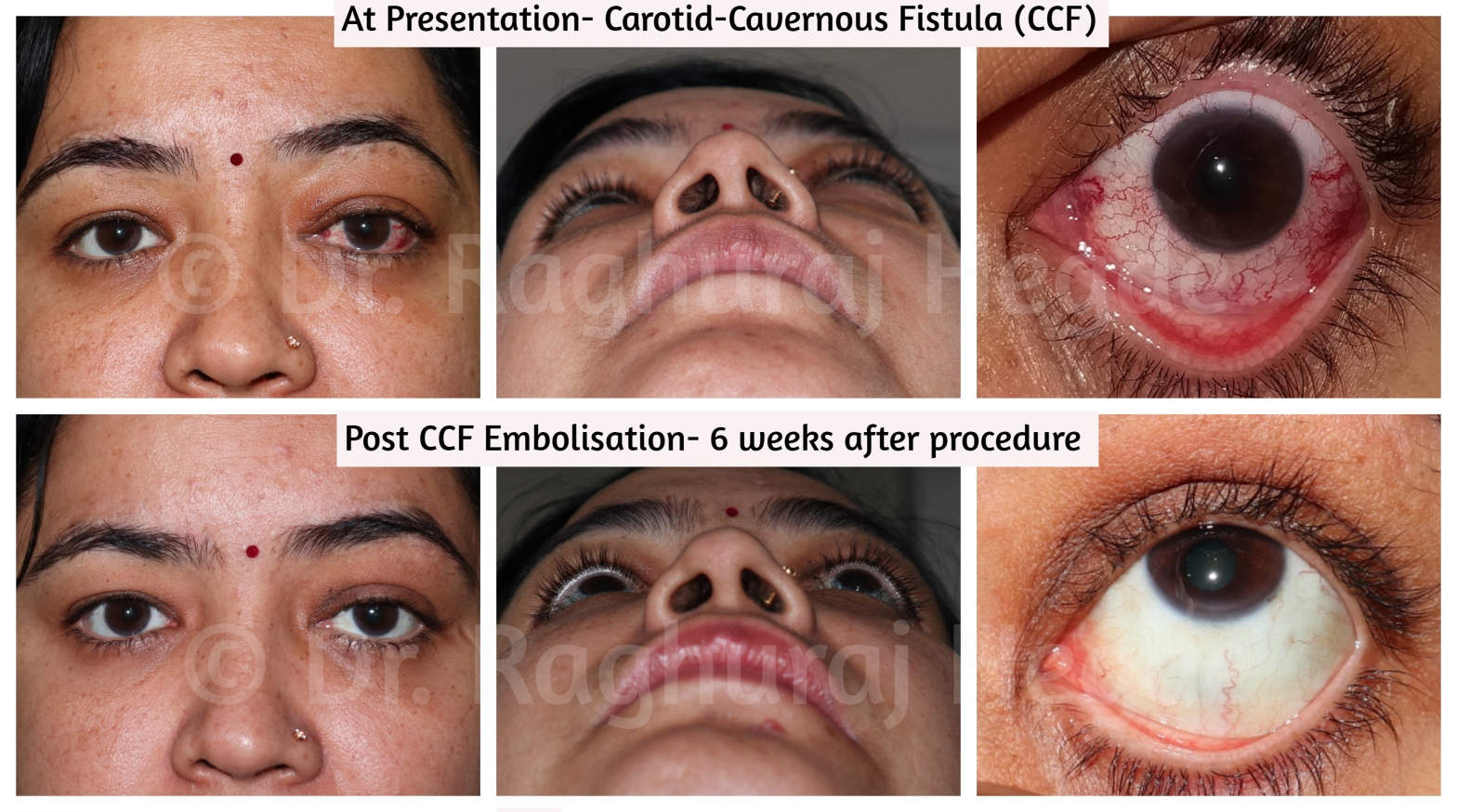
The case we are going to be discussing in this article is a 37 year old female patient who presented to the clinic with left eye
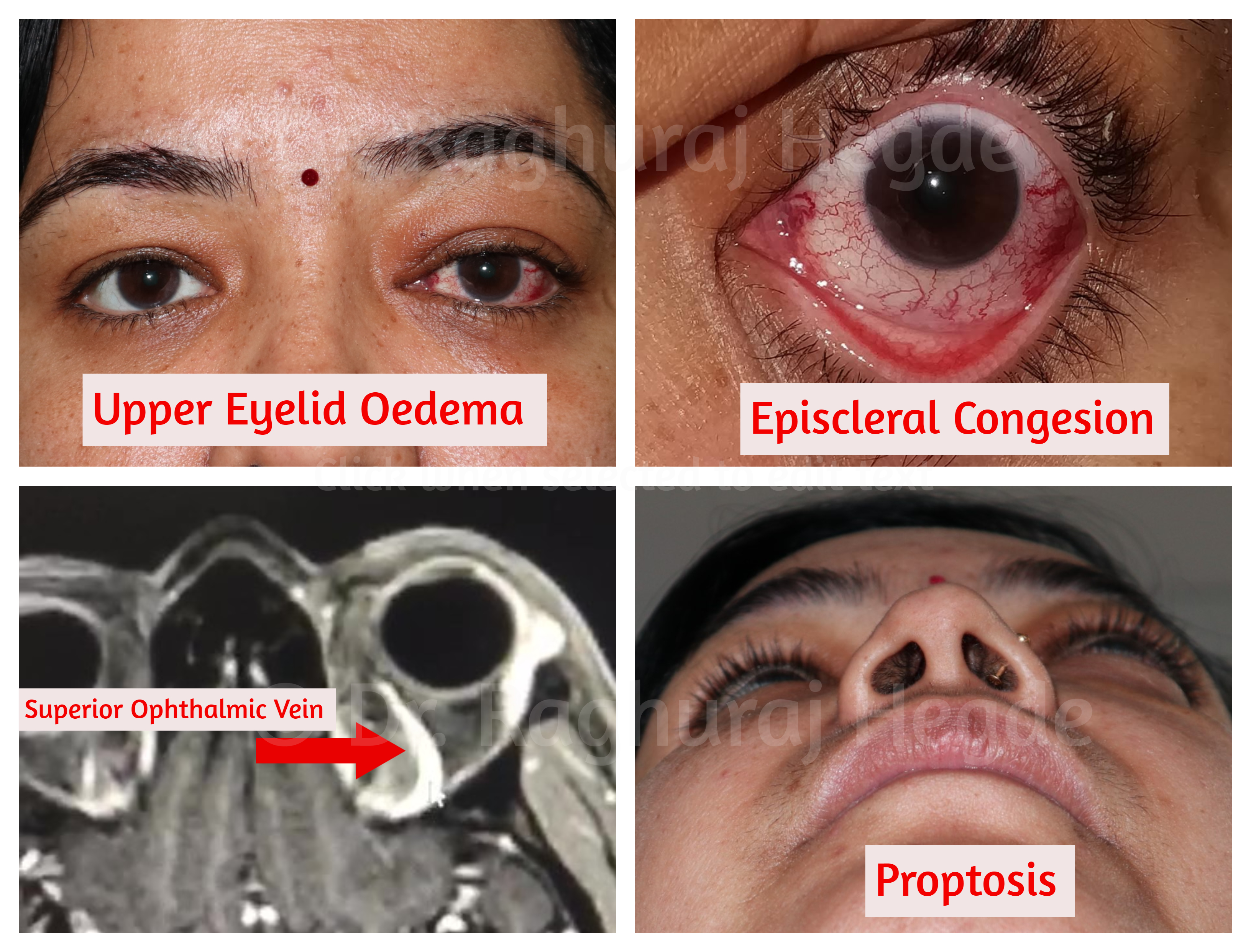
- Proptosis,
- Upper eyelid Oedema
- Engorged Episcleral Vessels
On examination she had
- Bruit on palpation
- Swooshing sounds on auscultation
- Increased intra-ocular pressure in the Left eye compared to Right (LE 21mmHg, RE 15mmHg)
A clinical diagnosis of Indirect Carotid-Cavernous Fistula was made.
This usually a straightforward referral to my Endovascular neurosurgery & Interventional Radiology colleagues who do an elegant minimally invasive procedure to close the CCF through the Femoral Vein. They got a Dynamic MRI, Digital Subtraction Angiography and Orbital Colour doppler to see flow. On the MRI You can see the superior ophthalmic Vein quite prominently because it has been arterialised (Red Arrow)
The DSA confirms the clinical diagnosis as well as the possible approaches to the cavernous sinus
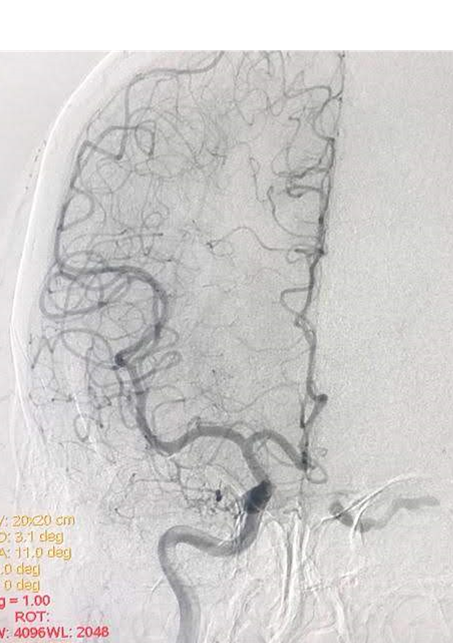
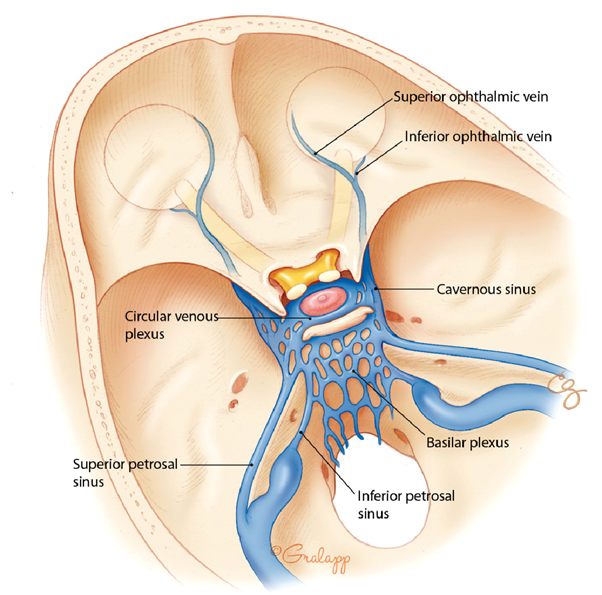
My Endovascular Neurosurgeons & Interventional Neuro-radiologist colleagues usually cure this condition in an elegant way running the angio- catheter through the femoral vein and accessing the CCF through the Inferior Petrosal Vein. Although the inferior petrosal sinus is the simplest, shortest, and most commonly used venous route to the cavernous sinus, the superior ophthalmic vein (SOV), superior petrosal sinus, basilar plexus, and pterygoid plexus present other endovenous options.
In rare instances, the SOV is the sole route available as in this case. Hence I was called upon to expose the SOV for my colleagues to gain access to the CCF. Hence I was called upon to expose the SOV for my colleagues to gain access to the CCF.
Exposure of Superior Ophthalmic Vein (SOV)
A medial eyelid crease incision. The Orbital Septum is then dissected and incised. Fat prolapses. Blunt dissection of the supero-medial orbital fat is done towards the supra-orbital notch till the arterialised SOV is identified (Blue Arrow). Once identified and dissected, the SOV is looped with a rubber ligature.
After SOV is identified it is followed by cannulation of the SOV and closure of the CCF using Onyx- a vascular embolic agent.
Six weeks post procedure there is complete disappearance of Left Eye Proptosis, Upper eyelid Oedema & engorged episcleral veins. The comparison photos at presentation and 6 weeks post embolisation of CCF.

It is very rare that oculoplastic surgeons are asked to provide access to interventional neuro-radiologists. This is one such case. We have performed such interventions in 3 cases till date at our hospital with similarly successful outcomes. The important thing to remember as a surgeon while accessing the SOV is that the vein is arterialised due to the CCF and bleeding can be very severe is the vessel wall is damaged. Hence three important factors in the successful outcome of this approach is
- Knowledge of Clinical Anatomy and the intimate relationship between the SOV and the other orbital tissue.
- Clean dissection field and careful movements in the supero-medial orbit.
- Delicate separation of orbital tissues from the SOV without damaging the vessel wall.
This case was interesting way to tackle the case. In a sense I was re-learning an old skill since this technique has been mentioned in literature for more than 30 years but due to advanced endovascular technology, this approach has run into disuse. As I found out, there may be certain candidates for this procedure.
References:
