

Since the fall and break-up of the Soviet Union, Mongolia’s healthcare has emerged as a free-market healthcare model. It has been struggling to transition from a state-run public healthcare to free market private healthcare enterprise. They have very eager doctors but have been lacking in training & mentorship. The present generation of ophthalmologists are breaking the mould. They have been travelling to other countries to gain expertise and returning to their home country to provide service. They have a genuine thirst for international interaction and collaboration.
Tag Archives: Eyelids
How do you correct hereditary acquired droopy eyelids?

Chronic progressive external ophthalmoplegia (CPEO) describes an spectrum of hereditary myopathies affecting extraocular muscles (EOMs) commonly manifesting as bilateral ptosis and near total external ophthalmoplegia.
As the name suggests, it is a chronic, progressive, bilateral, typically symmetric, and external (i.e., spares the pupil) ophthalmoplegia. CPEO is associated with mitochondrial disease and can occur as isolated oculomotor symptoms (isolated CPEO) or in conjunction with other systemic findings (“CPEO-plus”). Depending on additional clinical features, CPEO can be evaluated as part of a systemic myopathic or neurologic syndrome
Catching the Moving Lid!

Ocular Myasthenia Gravis (OMG) is one of the conditions that an oculoplastic surgeon can correct without surgery or any invasive intervention. It is a very satisfying to treat a patient of OMG provided the diagnosis is accurate. It has the rare distinction of being both under-diagnosed and over-investigated in different settings. Clinical examination is the cornerstone of a diagnosis of OMG. The various fancy but expensive testing can only corroborate a strong clinical suspicion
Your eyes reflects your personality

Ptosis can be easily treated with a day care, single sitting surgery and sometimes there need not even be a external skin incision. The surgery is known as conjunctivo-mullerectomy where the ptosis (droopy eyelid) is corrected using an incision on the wet surface of the eyelid.
Riding up the Lower lid!

Entropion is in common language inward turning of the eyelid margin. This causes trichiasis (lash-cornea touch), where the eyelashes are directed inwards toward the globe. This malposition can cause corneal irritation due to constant touch by the lashes.
An Eye for an Eye!

Hering’s Law for the eyelids: There is reflexive descent of the contralateral upper eyelid after the ipsilateral surgical correction of unilateral ptosis. Hering’s law is explained by considering the two eyes as paired organs and it follows that the muscles moving it will work in co-ordination.
Opening the window to the World

Droopy Eyelid Surgery or Ptosis correction surgery is more art than science. I’m sure all Oculoplastic Surgeons agree it is a challenge to treat patients with ptosis. Each case is so different that it is almost feels like you are starting from scratch. While challenging, it is also among the most satisfying Oculoplastic conditions to treat.
The Scar Cocktail!

Facial Trauma can be damaging with tissue loss. Despite accurate and meticulous reconstruction, the scarring can be severe in the face. Scar modulation is an essential part of post trauma care and I often advise patients as much when they come with traumatic injuries of the face.
The Hooded Eyelids!

After ruling out any connective tissue disorder which could also cause such a condition, I performed the Lateral Canthoplasty (Reconstructing the lateral canthus) thus restoring the ideal almond shape of the palpebral (eyelid) opening. Not just a new lateral canthus needs to be reconstructed, we also have the make sure the eyelid do not stick back together by using silicone bolsters as tissue spacers.
Finding a road to the fistula
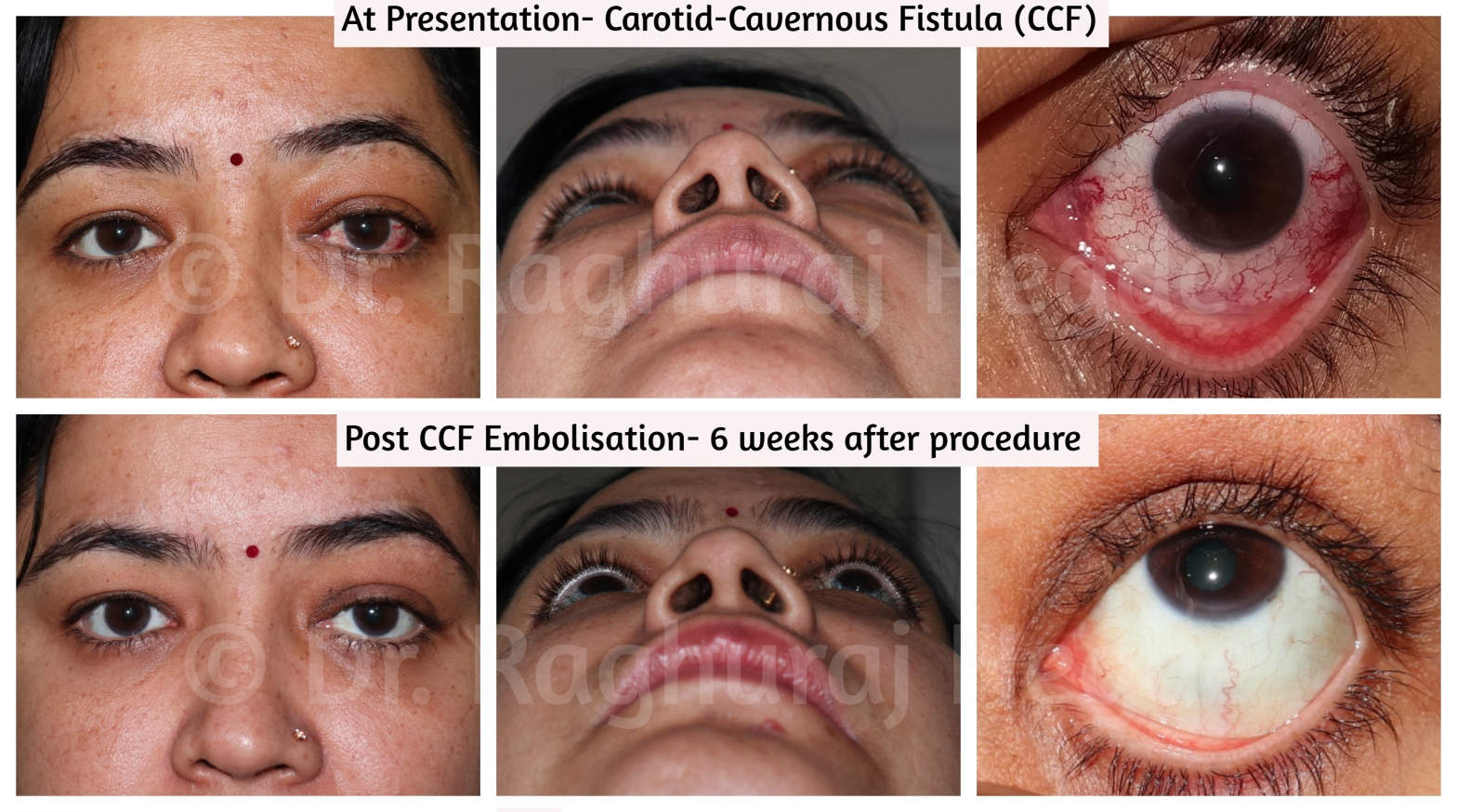
It is very rare that oculoplastic surgeons are asked to provide access to interventional neuro-radiologists. This is one such case. We have performed such interventions in 3 cases till date at our hospital with similarly successful outcomes. The important thing to remember as a surgeon while accessing the SOV is that the vein is arterialised due to the CCF and bleeding can be very severe is the vessel wall is damaged.
